Background & Introduction: Substance use history is often a major concern in the evaluation of heart transplantation (HT) candidates, as it has been associated with unfavourable outcomes. This includes challenges in adherence to medical regimens, engagement in inadequate self-care practices, and increased risk of morbidity and mortality. However, evidence regarding post-HT outcomes for this population remains inconsistent, likely due to small sample sizes and the lack of assessment of major clinical confounders. Assumptions and biases against patients with substance use disorder affect their likelihood of being listed for heart transplantation—a life-saving intervention—and thus raises ethical concerns. The aim of this study is therefore to compare HT outcomes of patients with and without substance use disorders in terms of mortality, hospitalization, and organ rejection rates, while adjusting for major confounding variables.
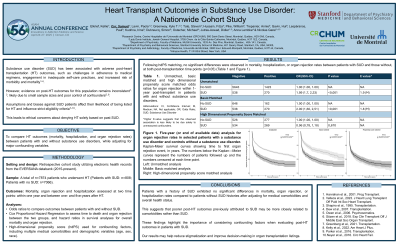
Methods: This is a retrospective cohort study with data from electronic health records from the EVERSANA databank—a dataset of over 120 million patients in the United States (2015-present). Mortality, organ rejection, and hospitalization were assessed at two-time points: within one year and between one—and five years after transplantation. Odds ratios were used to compare outcomes between patients with and without substance use disorder, while cox proportional hazard regression was used to assess time to death and organ rejection between the two groups. High-dimensional propensity score (hdPS) matching was used for confounding factors, including comorbidities (Charlson Comorbidity Index) and demographic variables (age, sex, race).
Results: The study included a total of n=7874 patients who underwent HT (substance use disorder: n=808 and control: n=7066). Patients were predominantly male (68.5%) with a mean age (SD) of 54.6 years (14.9). Prior to hdPS matching, our analyses revealed significantly higher rates of 13 out of 17 comorbidities in patients with a history of substance use. Following hdPS matching analyses, the control and exposed groups exhibited no significant differences in nearly all variables. Analyses revealed no significant differences in mortality, hospitalization, or organ rejection rates (p> 0.05) between patients with and without substance use disorders, but only when appropriately matched on key variables at both post-transplant time points.
Conclusion & Discussion: Patients with a history of substance use exhibited no significant differences in mortality, organ rejection, or hospitalization rates compared to patients without substance use after adjusting for medical comorbidities and overall health status. This suggests that poorer post-HT outcomes previously attributed to substance use may be more closely related to baseline comorbidities rather than substance use. These findings highlight the importance of considering confounding factors when evaluating post-transplant outcomes in patients with substance use. Our results may help reduce stigmatization and improve decision-making in organ transplantation listings.
References: 1. Dew MA, DiMartini AF, De Vito Dabbs A, et al. Rates and Risk Factors for Nonadherence to the Medical Regimen After Adult Solid Organ Transplantation. Transplantation. 2007;83(7):858. doi:10.1097/01.tp.0000258599.65257.a6 2. Hanrahan JS, Eberly C, Mohanty PK. Substance abuse in heart transplant recipients: a 10-year follow-up study. Prog Transplant. 2001 Dec;11(4):285-90. doi: 10.1177/152692480101100410. PMID: 11871277. 3. Owen JE, Bonds CL, Wellisch DK. Psychiatric evaluations of heart transplant candidates: predicting post-transplant hospitalizations, rejection episodes, and survival. Psychosomatics. 2006;47(3):213-222. doi:10.1176/appi.psy.47.3.213 4. Shapiro PA, Williams DL, Foray AT, Gelman IS, Wukich N, Sciacca R. Psychosocial evaluation and prediction of compliance problems and morbidity after heart transplantation. Transplantation. 1995;60(12):1462-1466. doi:10.1097/00007890-199560120-00016 5. Velleca A, Shullo MA, Dhital K, et al. The International Society for Heart and Lung Transplantation (ISHLT) guidelines for the care of heart transplant recipients. J Heart Lung Transplant Off Publ Int Soc Heart Transplant. 2023;42(5):e1-e141. doi:10.1016/j.healun.2022.10.015
Learning Objectives:
Understand the concern associated with a substance use history in the evaluation of heart transplantation candidates.
Realize the evidence regarding post-heart transplant outcomes for patients with substance use disorder remains inconsistent
Appreciate that after adjustment for medical comorbidities, patients with a history of substance use exhibited no significant differences in mortality and organ rejection rates compared to patients without substance use